Thank you everyone who participated and helped facilitate our Renal SG sessions this Thursday 1/25. As promised, teaching points are below.
SG Stations:
- Renal US review.
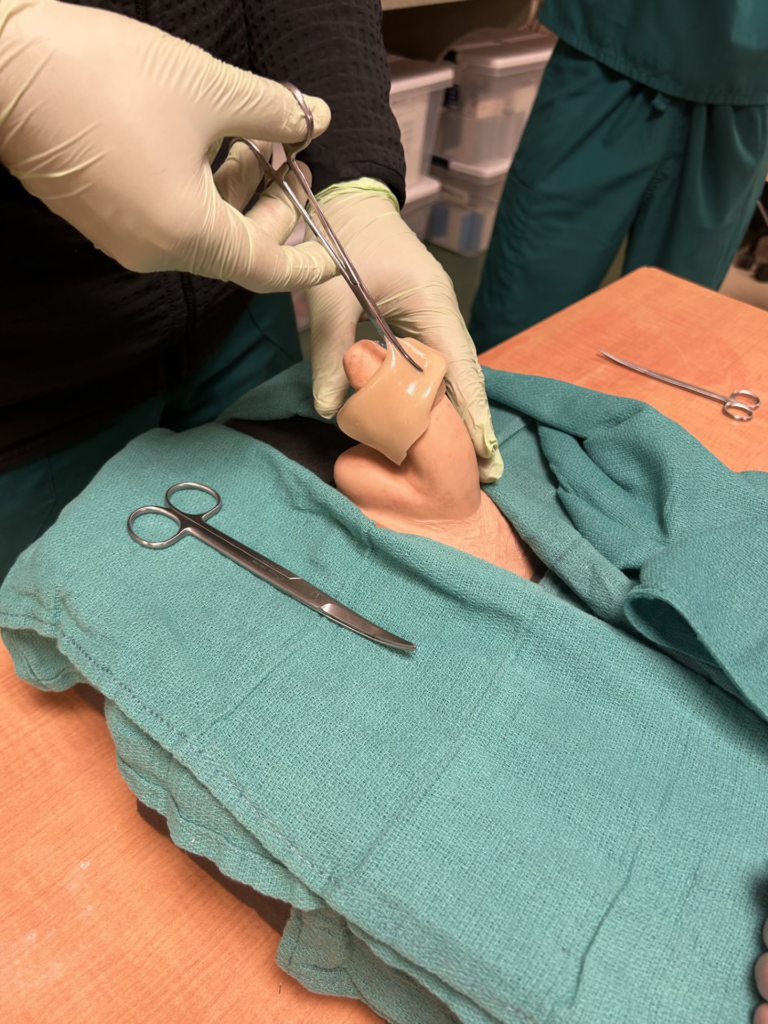
- Priapism drainage, Dorsal slit for paraphimosis.
- Multifactorial metabolic acidosis case including salicylate overdose.
- Hyponatremic seizure in a pediatric patient.

Case: Multifactorial Metabolic Acidosis
This was a 60F presenting altered after a week of GI symptoms. Baseline of T1DM on insulin as well as GERD taking PRN pepcid and pepto-bismol (the pink stuff from costco). She was found to have an Anion Gap Metabolic Acidosis (AGMA) as well as with a severe AKI. The cause of this was multifactorial with element of DKA, dehydration, uremia and salicylate overdose. The acute renal injury with increased use of pepto-bismol resulted in the salicylate overdose. Ultimately dispositioned to the ICU for dialysis.
Teaching Points:
- – Unintentional overdose should be considered in AMS workup especially in elderly.
- – Pepto-Bismol = Bismuth Subsalicylate.
- – Salicylate overdoses can lead to pulmonary edema and spectrum of neurological compromise from confusion to seizures to coma. Uncoupling of oxidative phosphorylation leads to high lactate levels.
- – Salicylate overdoses can be acute or chronic. Therapeutic range 15-30 mg/dL.
- – Since salicylates are renally excreted. Overdose can be exacerbated by acute kidney injury like in this case. Salicylate overdose also in itself causes renal injury.
- – Classic tinnitus may not be obvious in elderly, can be decreased hearing or even auditory hallucinations.
- – Consider dialysis if:
- – Urinary Alkalization is not feasible.
- – Severe toxicity with neurological compromise, renal failure, acidemia.
- – Urinary Alkalization is not feasible.
- Today’s AGMA is a classic board Q for both upcoming ITE as well as the boards:
- Relevant VBG and BMP numbers from today: pH 7.2. AG 22. CO2 23. HCO3 16.
- Is this only a metabolic acidosis?
- Winter’s Formula: Expected PaCO2 = 1.5 x (serum HCO3) +8
- Expected PaCO2 = 1.5 x (16) + 8 = 32
- Measured CO2 = 23
- Acute toxicity >80-100mg/dL – lower threshold if chronic toxicity.
Lower measured CO2 implies Concomitant Primary Respiratory Alkalosis
- Is there another metabolic disturbance?
- Delta gap = Measured anion gap – normal anion gap = 22 – 12 = 10
- Corrected HCO3 = delta gap + measured serum HCO3
- [24] = [10] + [14] à Corrected HCO3 = Normal HCO3!
- No other concomitant metabolic acidosis or alkalosis
- This patient had a Primary Metabolic Acidosis with Primary Respiratory Alkalosis
- Salicylate overdose causes concomitant primary respiratory alkalosis due to central stimulation of respiratory drive, not just a response to acidosis.
- The AGMA itself was driven by combination of dehydration, uremia, mild DKA as well as the salicylate overdose. If lactic acid had been repeated it would have risen from 5.5 to 7.0 despite fluid resuscitation. This should be a clue that there may be more going on. Keep those differentials wide!

Case: Pediatric Hyponatremic Seizure
This was a 10M presenting after a seizure during a sports meet. Found to be hyponatremic (122) in the setting of recent initiation of desmopressin for bedwetting. Combination of desmopressin and increased free water intake during a day of outdoor exercise led to the seizure. Received hypertonic saline and dispositioned to the PICU.
Teaching Points:
- Desmopressin is a synthetic analogue of vasopressin. It stimulates re-absorption of free water at the level of the collecting ducts by insertion of aquaporin channels. This can cause hyponatremia.
- Intra-nasal desmopressin is sometimes prescribed to children with bedwetting issues. Administered at night to decrease urine production.
- Hyponatremia exacerbated in this case due to significant increase in free water intake at sporting event on a particularly hot day.
- Initial symptoms of hyponatremia typically involve nausea and malaise (Na 120-130). At lower levels (Na <120) this can progress to AMS, lethargy, seizures, coma, pulmonary edema, cardiac arrest.
- The rate of decrease in sodium is most important. With an acute drop, worse symptoms can develop with seemingly less severe levels of hyponatremia.
- Initial bolus of 3% hypertonic saline typically ranges from 100-250mL over 10 minutes in adults.
- In pediatrics, consider a 3ml/kg bolus (max 250-300mL) over 30 minutes.
- Hypertonic saline has a rapid onset of action in ~10 minutes. Consider an additional bolus after 10-15 minutes if needed.
- The dreaded osmotic demyelination syndrome due to hyponatremia overcorrection should be considered in patients who may have severe hyponatremia in subacute to chronic timeframe. Adaptation process takes about 2 days.
- Consider hypertonic saline in patients with significant symptoms (seizures, AMS with vomiting).
- In general sodium should not be raised more than 10-12mmol over 24 hours and the daily rate of increase is more important than the hourly rate of increase.